Transforming Patient Intake with AI Resulting in 23% Cost Saving
Product Overview
Client Overview
A mid-sized multi-speciality hospital in western India, serving over 800 outpatient visits per day across six departments. Dermatology, orthopaedics, and general medicine account for approximately 70% of OPD volume. The hospital operates across two campuses with a central front-desk team of nine full-time staff handling all patient intake across three shifts.
Over the past two years, OPD volume had grown by 22%. Headcount had grown in step, but efficiency had not. By early 2024, the leadership team recognised that continuing to add staff was no longer a viable response to growth.
Business Challenge
The hospital's intake operations had three distinct, measurable problems.
1. Front-Desk Capacity Was a Bottleneck
Nine front-desk staff were collectively managing approximately 320 intake-related tasks per day: patient registration, insurance pre-verification, phone inquiries, WhatsApp responses, slot coordination, and follow-up calls. During the morning peak (9 am to noon), all three front-desk counters ran at full utilisation with queues regularly forming.
Manual data entry was the primary source of errors. Staff were transcribing patient details from phone calls and WhatsApp messages into the hospital information system (HIS), which resulted in an average of 22 rescheduling events per week caused by duplicate records, mismatched contact numbers, or incorrect department assignments. Each rescheduling event consumed roughly 15 minutes of staff time to resolve.
When OPD volumes spiked — during monsoon, festive weeks, or after a referral drive — the only lever available to management was authorising overtime. There was no elasticity in the system.
2. After-Hours Demand Was Being Lost
An internal analysis of missed calls and unresponded WhatsApp messages over a four-week period revealed the following:
• Approximately 35 patient inquiries arrived daily between 7 pm and 9 am — outside staffed hours.
• Of these, fewer than 40% resulted in a booking the following morning. The remainder either did not follow up or could not be reached.
• A spot survey of 60 patients who had inquired but not booked found that 58% had booked at another facility within 24 hours of their initial inquiry.
This represented a consistent daily loss of approximately 21 bookings. At an average OPD revenue of ₹650 per visit, the opportunity cost was approximately ₹13,650 per day — or roughly ₹40 lakh per quarter — excluding downstream diagnostic and pharmacy revenue.
Appointment slot utilisation, measured across all departments, averaged 61% against a target of 80%. Dermatology was the worst performer at 54%, largely because its slots required advance booking, which patients initiated in the evening.
3. Management Had No Intake Funnel Visibility
The intake process generated no structured data. The COO's team could report total OPD visits per day, but could not answer the following questions with any accuracy:
• What percentage of inquiries converted to confirmed appointments?
• At which step were patients dropping off — initial inquiry, slot selection, or confirmation?
• Which departments had the highest no-show rates, and on which days?
• How much front-desk time was spent on administrative follow-up versus live patient interaction?
Without this data, operational decisions — staffing levels, doctor scheduling, marketing spend — were based on intuition rather than evidence. When the leadership team proposed an efficiency initiative, they had no baseline against which to measure improvement.
Solution Overview:
The core architecture consisted of following components:
Component | What it does | Scope |
Patient intake bot | WhatsApp chat in Multiple languages | New and returning patients; OPD across all specialities |
Identity verification | Phone number check against hospital HIS via REST API | Eliminates duplicate records; reduces manual data entry |
Slot booking engine | Real-time read/write to scheduling system; doctor-level availability | Doctor's schedule managed effectively |
Reminder automation | 48-hr reminders + 2-hr WhatsApp reminder; 1-tap confirm or reschedule | Sent for all confirmed appointments across all departments |
Human escalation | The bot hands off to the front-desk agent when the confidence score < 70% | Covers complex queries, insurance questions, and emergency triage |
Management dashboard | Live KPIs: intake volume, conversion funnel, slot utilisation, staff load | Accessible to COO, department heads, and front-desk supervisors |
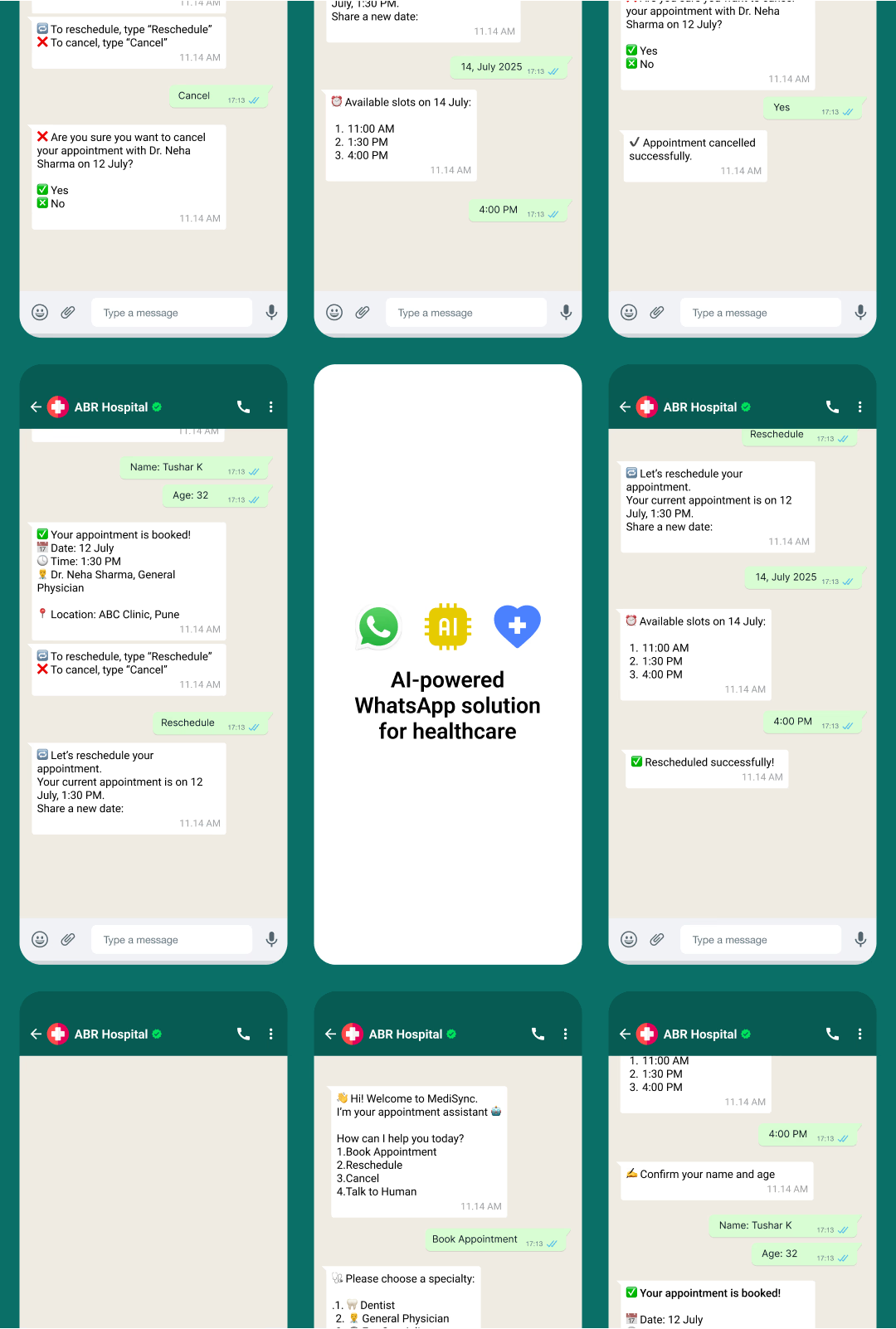
Before the platform, a new patient calling after hours would reach a voicemail or an unanswered line. The next morning, a staff member would attempt a callback — often two to three hours into the working day. By that point, the patient had frequently already booked elsewhere.
Post-deployment, the same patient receives an immediate WhatsApp response from the intake bot. Based on the patient's language preference, the bot collects their name, phone number, reason for visit, and preferred time. It verifies their UHID against the HIS (or creates a new record if they are a first-time patient), surfaces available slots in real time, and confirms the booking with a calendar entry and SMS confirmation within approximately four minutes on average.
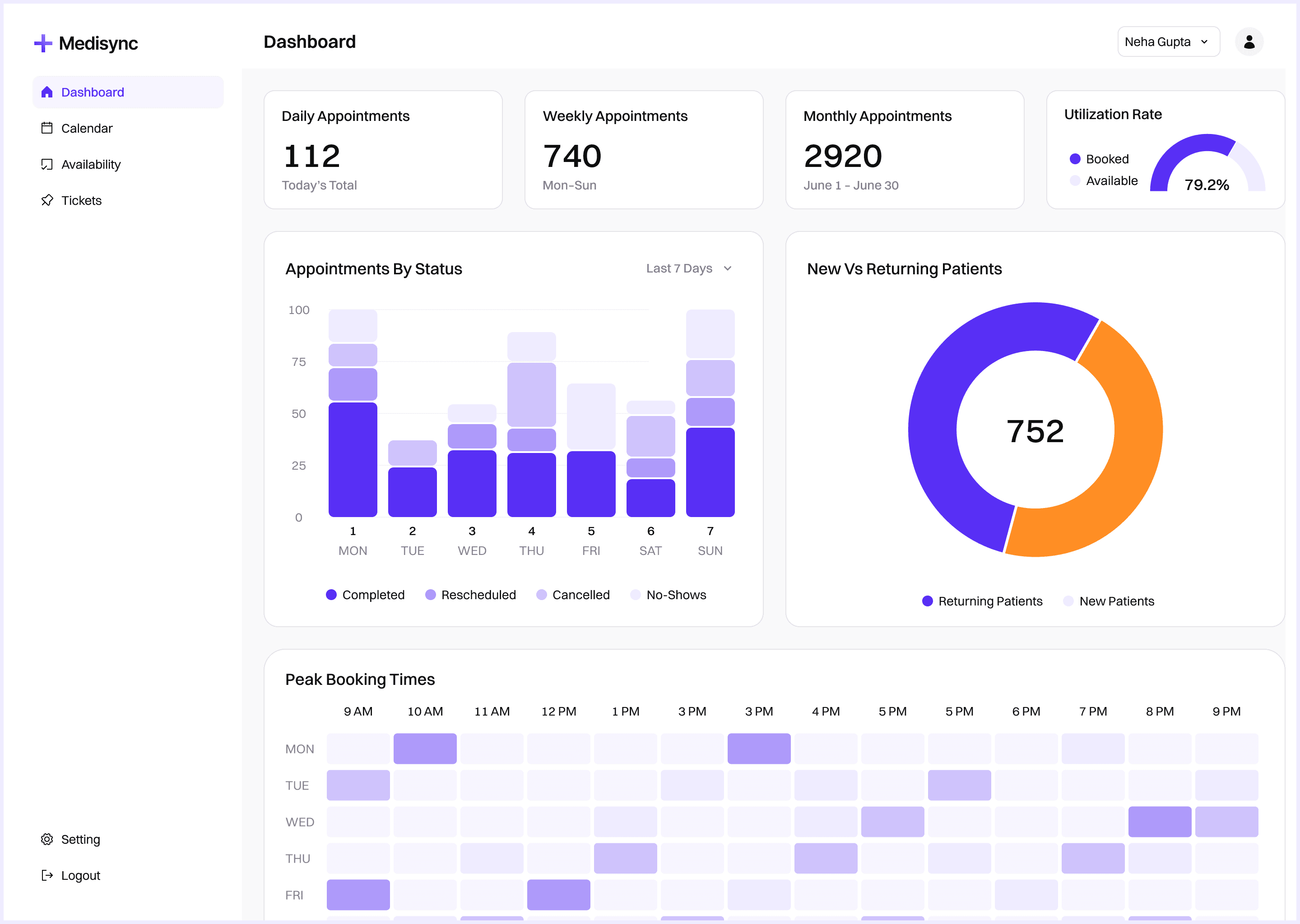
Operational Impact and Outcome:
Outcomes were measured at 30, 60, 90, and 180 days post-go-live, benchmarked against the four-week baseline period preceding deployment.
Metric | Before | After | Timeframe |
After-hours inquiry capture | ~15% | ~78% | Within 60 days |
Appointment slot utilisation | 61% | 76% | Within 90 days |
Inquiry-to-booking conversion | 38% | 57% | Within 90 days |
Patient no-show rate | 18% | 11% | Within 120 days |
Front-desk headcount | 9 FTE | 9 FTE (flat) | Despite +22% OPD volume |
After-hours booking availability | 0 hours | 24/7 | Day 1 post-go-live |
Slot utilisation improvement from 61% to 76% was the single largest revenue-side outcome. Across all departments, this represented approximately 120 additional confirmed appointments per week that would previously have gone unfilled. At an average OPD revenue of ₹650, this added roughly ₹78,000 per week in direct OPD revenue — before downstream diagnostic and pharmacy uplift.
Implementation Journey
How we bring your vision to life
Process & Cost Diagnostics
AI System Design
Deployment & Change Management
Evaluation & Enhancement
Process & Cost Diagnostics
AI System Design
Deployment & Change Management
Evaluation & Enhancement
Integration & Compliance
WhatsApp Integration
IVR Telephony Integration
DPDP Compliance

Scale of Application
23%
reduction
in operational cost
42%
Reduction
in patient waiting time
31%
INCREASE
in lead to appointment conversion
90%
ACCURACY
of automated patient intake